
















 43 96
43 96

proinflammatory
cytokines
such
as
interleukin
(IL)-1
b
,
IL-6,
and
tumor
necrosis
factor-
a
.
All
these
detrimental
effects
are
prevented
by
inhibiting
nicotinamide
adenine
dinucleotide
phosphate
oxidase
or
by
using
antioxidant
agents
[15] .To date,
less
robust evidence exists
regarding
the effects
of
smoking
on
neuronal
nitric
oxide
synthase–mediated
penile erection and on
inducible nitric oxide
(iNOS) activity
and
expression
[13].
From
a
clinical
standpoint,
numerous
studies
have
shown
that
smoking
exposure
leads
to
impaired
arterial
flow
to
the penis or
acute
vasospasm
of
the penile
arteries.
For
instance,
the
relative
risk
of developing
atherosclerosis
in
the
penis
and
subsequent
ED
is
1.31
for
each
10
pack-
years
smoked
[16],
and
86%
of
smokers
have
an
abnormal
penile vascular evaluation
[17].
Furthermore, penile
rigidity
during
nocturnal
erection
inversely
correlates
with
the
number
of
cigarettes
smoked
per
day
[18].
Pathophysiologic
biochemical
and
clinical mechanisms
involved
in
the
causal
relationship
between
smoking
and
erectile
dysfunction
are
outlined
in
Figure 2 .3.2.
Erectile
dysfunction
and
smoking:
dose–response
relationship
3.2.1.
Smoking
quantity
In
the most
recent
dose–response meta-analysis,
Cao
et
al
evaluated
the
association
of
quantity
and
duration
of
smoking with
ED
[19].
One
cohort
study
and
nine
cross-
sectional
studies
were
included
in
the
meta-analysis
(50
360
participants
and
12
218
cases
with
ED).
The
authors
found
the
risk
for
an
increment
of
10
cigarettes
smoked per day and 10 yr of
smoking was
increased by 14%
and
15%,
respectively.
The
summary
OR
of
ED
for
an
increase
of 10
cigarettes
smoked per day was 1.14
(95% CI,
1.09–1.18),
with
moderate
heterogeneity
(
p
= 0.061;
I
2
= 44.7%).
For
an
increment
of
10
yr
of
smoking,
the
combined ORs
of
ED was
1.15
(95% CI,
1.10–1.19), without
substantial heterogeneity
(
p
= 0.522;
I
2
= 0.0%). No evidence
of a curve
linear association was observed between smoking
and
risk
of
ED.
However, most
of
the
studies
were
cross
sectional,
and
the
methods
used
to
diagnose
ED
were
different
across
the
included
studies.
In
a
study by He
et
al,
there was a
statistically
significant dose–response
relation-
ship
between
smoking
and
the
risk
of
ED
(
p
= 0.005).
Multivariate-adjusted
ORs
of
ED
were
1.27
(95%
CI,
0.91–1.77),
1.45
(95%
CI,
1.08–1.95),
and
1.65
(95%
CI,
1.08–2.50)
for
those
who
smoked
1–10,
11–20,
and
>
20
cigarettes
per
day,
respectively,
compared
with
never
smokers
[9].
A Canadian study by Polsky et al
found
that men with ED
were
twice
as
likely
to be
former
smokers
(OR: 2.2; 95% CI,
1.2–3.9),
and
cumulative
smoking
in pack-years
suggests
a
dose–response
pattern with
the
risk
of
ED
[20].
Parazzini
et
al
performed
a
cross-sectional
study
to
analyze
the
prevalence
and
risk
factors
for
ED
in
Italy.
In
comparison with never
smokers,
the OR of ED was 1.7
(95%
CI, 1.2–2.4)
for current smokers and 1.6
(95% CI, 1.1–2.3)
for
former
smokers
and
increased with
duration
of
the
habit
[21].
Evaluating
smoking
as
a
risk
factor
for
ED
in
9670 men
with
diabetes,
Bortolotti
et
al
found
the
ORs
of
ED
in
comparison with
never
smokers was
1.4
(95%
CI,
1.3–1.6)
for
smokers
and
1.5
(95%
CI,
1.3–1.6)
for
former
smokers.
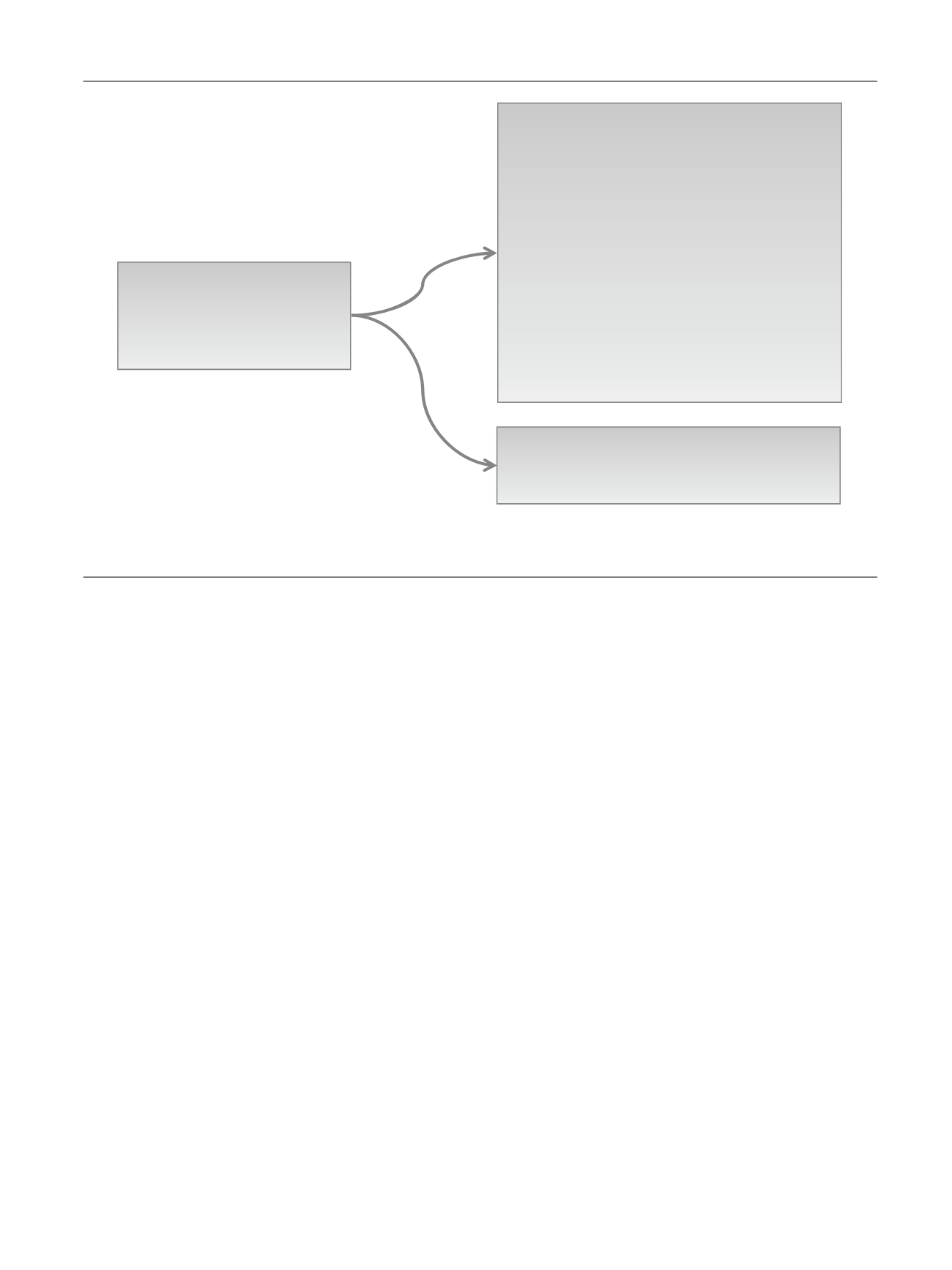
Detrimental effects
of
cigareƩe
smoking
CLINICAL MECHANISMS
-
Severe
atherosclerosis
leading
to
penile
impaired
arterial
flow
and
acute vasospasm oŌ he penile arteries
BIOCHEMICAL MECHANISMS
Endothelial
impairment
- Decreased eNOS
acƟvity
-
Impaired
endothelium-dependent
vasorelaxaƟon
-
Increased
expression
of
cell adhesion
molecules
and
transendothelial migraƟon of monocyte-like
cells
- Reduced
response
to vascular
endothelial
growth
factor
-
Impaired
regulaƟon ofi mportanƩ hromboƟc
factors
-
Impaired
expression and
fucnƟoning
of
nNOS-mediated
penile
erecƟon and
iNOS expression
OxidaƟve damage
-
Imbalanced producƟon
of oxidaƟve and anƟoxidaƟve
agents
-
Increased
superoxide
generaƟon
by both
endothelial
and
smooth muscle
cells
-
Impaired
acetylcholine-induced
relaxaƟon of arteries
-
Increased mRNA
expression
of proinflammatory
cytokines
(IL-
1β,
IL-6, TNF-α).
Fig.
2
–
Pathophysiologic
biochemical
and
clinical mechanisms
involved
in
the
causal
relationship
between
smoking
and
erectile
dysfunction.
eNOS = endothelial
nitric
oxide
synthase;
IL =
interleukin;
iNOS =
inducible
nitric
oxide
synthase; mRNA = messenger RNA;
nNOS = neuronal
nitric
oxide
synthase;
TNF =
tumor
necrosis
factor.
E U R O P E A N
U R O L O G Y
F O C U S
1
( 2 0 1 5
)
3 9 – 4 6
43