
















 40 96
40 96

smoking
and
ED,
the
influence
of
smoking
on
ED
severity,
progression,
and
treatment
success
and
the
influence
of
smoking
cessation
on
the
restoration
of
normal
erectile
function
is
less
clear
[3] .The
aim
of
this
review
was
to
critically
analyze
the
relationship
between
ED
and
smoking
by
addressing
the
epidemiological
and
pathophysiologic
aspects
on
which
this
link
is
founded. We
focused
on
the
clinically
relevant
aspects of
this association,
trying
to clarify whether a dose–
response
relationship
exists
and
to
what
extent
smoking
cessation
affects
normalization
of
erectile
function.
2.
Evidence
acquisition
A
systematic
literature
review was
performed
in
October
2014
using Medline,
Embase,
and
Scopus
databases.
The
search
strategy
included
the
terms
smok*,
tobacco,
cig*,
erectile
dysfunction,
ED,
erectile
function,
impotence,
occur-
rence,
progression
,
and
response.
We
limited
our
search
to
prospective
trials
and major
preclinical
and
retrospective
studies
published
in
English
between
January
1998
and
October
2014. Meeting
abstracts,
editorials,
and
commen-
taries
were
excluded.
In
addition,
cited
references
from
selected
articles
and
from
review
articles
retrieved
in
our
search
were
used
to
identify
manuscripts
that
were
not
included
in
the previous
search. The
articles
that provided
the
highest
level
of
evidence
were
selected
with
the
consensus
of
all
the
authors. We
identified
4214
articles
from electronic databases after
the exclusion of duplicates.
Of
these,
most
were
excluded
after
the
first
screening
based
on
titles
and
abstracts
because
they
were
not
relevant
or
did
not
fulfill
the
inclusion
criteria.
After
evaluating
the
full
texts
of
110
remaining
articles
that
seemed
to
be
relevant
for
this
review, we
finally
included
13
studies
( Fig. 1).
2.1.
Data
extraction
Data
from all
selected
studies were extracted and
tabulated
by
one
author
(M.M.)
and
corroborated by
a
second
author
(P.V.).
The
p
values
were
recorded
for
relationship
of
smoking with
end
points,
and
statistical
significance was
defined
as
p
<
0.05.
If
p
values
were
not
available,
95%
confidence
intervals
(CIs) were
recorded. Wherever
avail-
able, hazard
ratios or odds
ratios
(ORs) were
also
recorded.
In
cases
in
which multiple
statistical
tests
were
used
to
assess an association,
results of
the most
rigorous
test were
reported
(eg, a multivariable analysis adjusting
for standard
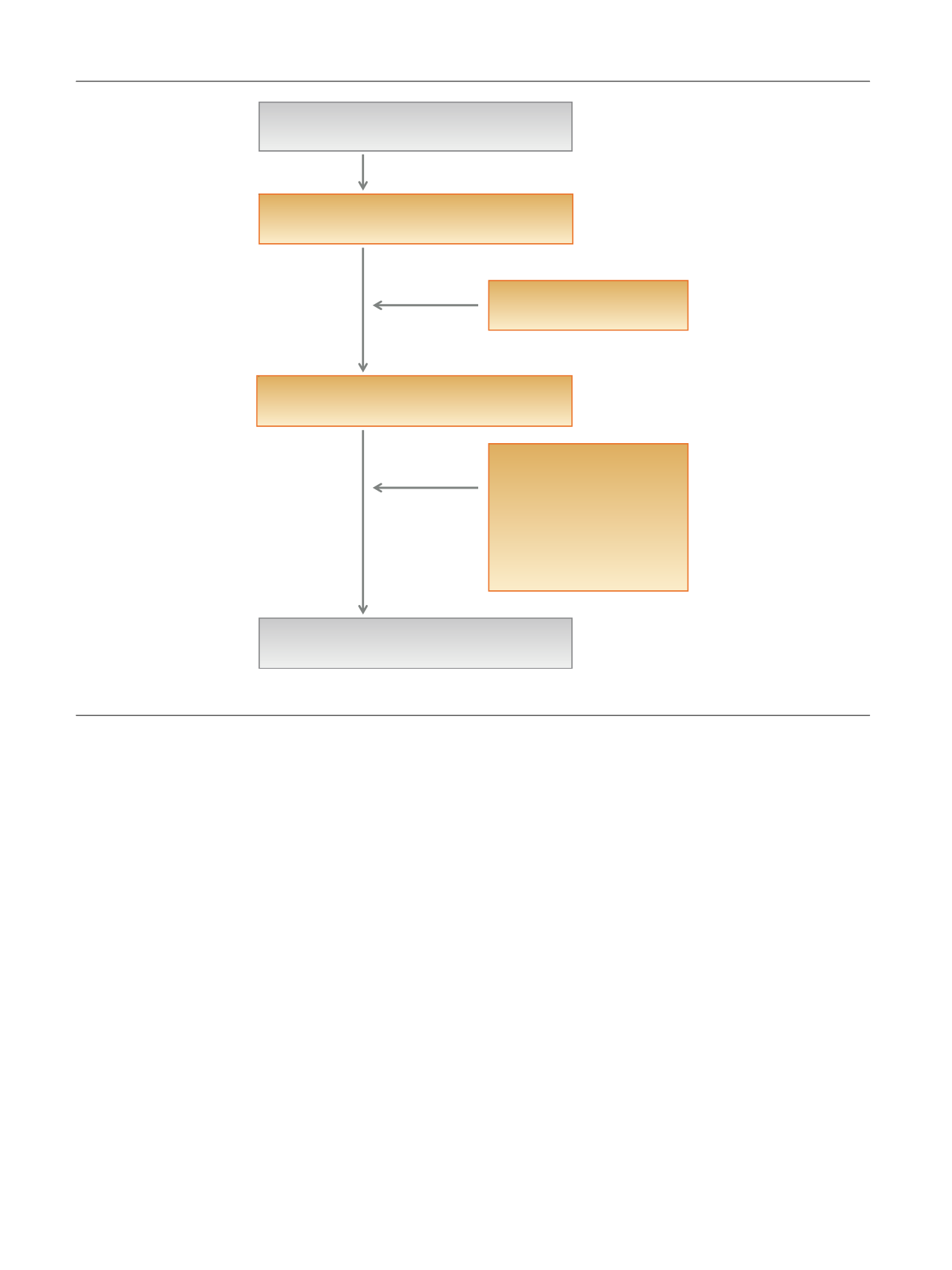
Records identified through PubMed, Embase, and
Scopus (
n
= 4214)
Records after duplicates removed (
n
= 3279)
Records excluded based on
abstract (
n
= 3169): not relevant
to this review
Records selected for full-text evaluation (
n
= 110)
Records excluded following full-
text accession (
n
= 97): review
articles, abstracts, editorials,
and meeting commentary; not
published in English; not
relevant to this review;
heterogeneous patients;
insufficient published case
studies
Papers included in this article (
n
= 13)
Fig.
1
–
Flowchart
of
study
selection.
E U R O P E A N
U R O L O G Y
F O C U S
1
( 2 0 1 5
)
3 9 – 4 6
40